Nevus sebaceous (Nevus sebaceous of Jadassohn) is a hamartoma with epidermal, sebaceous, and apocrine components that presents as a congenital patch located predominantly on the scalp. ICD-10 Code: Q85.9.
In most cases, it's present at birth (about 0.03% of newborns) or later, in infancy and early childhood. The lesions change clinically and histologically with age. During puberty, sebaceous nevi enlarge, and it's often at this time that they first become noticeable. Hormonal changes during puberty stimulate the growth of sebaceous glands.
In most cases, the nevus develops sporadically, but it can also be inherited in an autosomal dominant manner. It has been found that postzygotic somatic mutations of the HRAS gene are observed in 95% of nevus keratinocytes and KRAS in 5%, causing increased cell proliferation and apparently predisposing to the development of secondary tumors within the nevus area.In almost 50% of cases, sebaceous nevus is localized on the head (scalp, forehead, centrofacial and peri-auricular regions) and on the genitals. Typically there's a single lesion. It presents as a linear or oval, slightly elevated plaque above the skin surface, hairless, with a color that may be yellow, orange, or flesh-colored, with a diameter of 1-3 cm. The lesion passes through three developmental stages corresponding to the stages of sebaceous gland maturation in childhood, during puberty and in adulthood.
Nevus Sebaceous in Childhood

Nevus Sebaceous in puberty

Nevus Sebaceous in adults

"SCALP" Syndrome

Nevus sebaceous remains stable during childhood and undergoes predictable changes during adolescence. Depending on its location, a sebaceous nevus may be disfiguring. Non-neoplastic changes often occur in adulthood, so preventive excision of the nevus during adolescence may be advisable in some children.
Approximately 20-25% of cases involve non-neoplastic changes:
- Benign Tumors: Over 80% of benign tumors form on the scalp. The most common (up to 40%) is syringocystadenoma papilliferum, followed by trichoblastoma, trichilemmoma, trichilemmal cyst, and apocrine adenoma.
- Malignant Tumors: Basal cell carcinoma is the most common malignancy, developing within nevus sebaceous in approximately 3-5% of cases. Nearly all cases of sebaceous carcinoma arising from a nevus are found in women and are not associated with Muir-Torre syndrome. Less common neoplasms include squamous cell carcinoma, apocrine carcinoma, eccrine porocarcinoma, leiomyosarcoma, malignant melanoma, and mucoepidermoid carcinoma.
The diagnosis is established based on the clinical presentation, dermatoscopy, and biopsy of the affected area.
Dermatoscopy: Pink-orange non-structured areas lacking hair associated with a whitish network.- Linear epidermal nevus
- Seborrheic keratosis
- Basal cell carcinoma
- Congenital aplasia of the skin
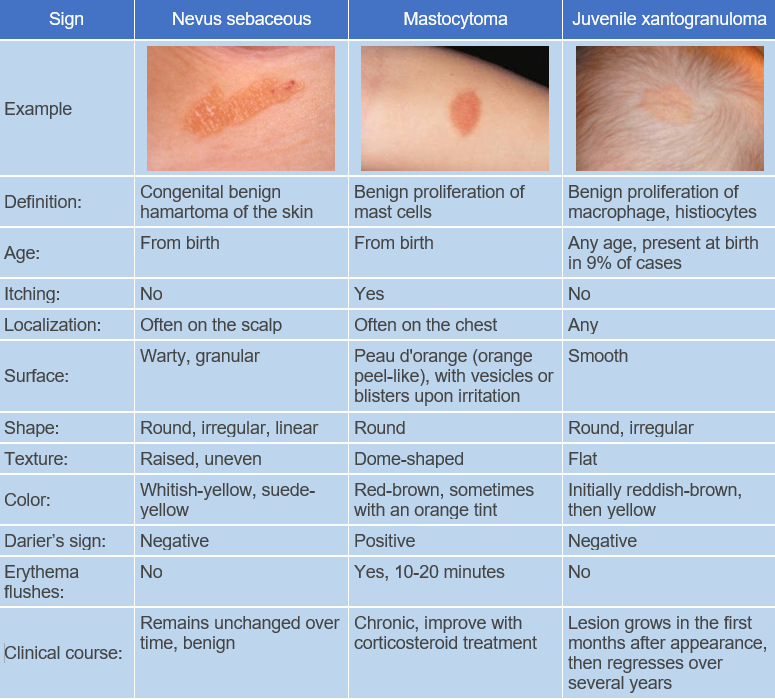
- Solitary mastocytoma
- Juvenile xanthogranuloma
- Nevus comedonicus
- Syringocystadenoma
- Melanoma
- Benign melanocytic nevus