Hirsutism is a condition in women in which terminal hair growth occurs in androgen-dependent areas, similar to what occurs in males after puberty. In other words, the term "hirsutism" applies only to women. ICD-10 Code: L68.0
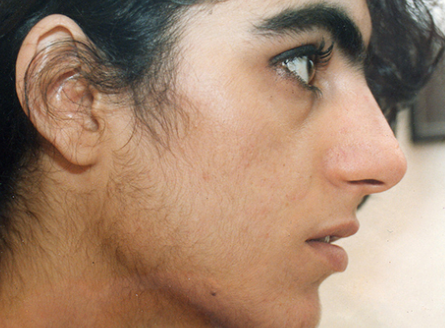
Androgen-dependent areas include the cheeks, upper lip, chin, chest, abdomen, inner thighs, back, and legs. In women, only vellus hair normally grows in these areas. There are significant differences in what is considered hirsutism depending on racial, cultural, and social factors. What may be considered pathological in Northern European women may be considered normal in Mediterranean women. Facial and body hair is less common in blacks, mongoloids, and Native Americans.
Hirsutism may occur for the following reasons: increased secretion of androgens, increased sensitivity of genital hair follicles to normal levels of circulating androgens, increased levels of free testosterone, or increased activity of 5-alpha-reductase. Circulating levels of androgens in women depend on their direct secretion by the ovaries and adrenal glands, as well as peripheral conversion of androgen precursors and the rate of metabolic clearance associated with androgen production. All of these conditions result in the conversion of vellus hairs to terminal hairs in sex hormone-sensitive follicles.
Idiopathic Hirsutism
The idiopathic cause is the most common. This condition is due to hypersensitivity of hair follicles to androgens, decreased levels of sex hormone-binding globulin, or increased activity of 5-alpha-reductase. This type of hirsutism is usually noticed during puberty, and in most cases there is a family history of hirsutism.
Ovaries
Polycystic ovary syndrome (PCOS): These patients present (usually just before or during puberty) with symptoms such as hirsutism, acne, dysfunctional uterine bleeding or amenorrhea, infertility, and obesity. In some cases, the pathology may not be manifest and the syndrome is detected by abdominal ultrasound.
Ovarian tumors: Functional ovarian tumors occur in less than 1% of all ovarian tumors. In these cases, hirsutism usually begins suddenly between the ages of 20 and 40 and progresses rapidly.
Adrenal Glands
Congenital adrenal hyperplasia (CAH): There are three types of CAH: a) severe form with masculinization at birth; b) milder form with masculinization in childhood in which girls are very tall at an early age but later have relatively normal height; and c) late onset form either at the time of puberty or during pregnancy. The most common enzyme deficiency in CAH is 21-hydroxylase deficiency, which accounts for 95% of all cases.
Adrenal tumors: These rarely cause hirsutism. They can occur at any age, but usually present before puberty or in the postmenopausal years. Symptoms are sudden and progress rapidly.
Prolactinoma
Prolactinoma: It can result from a pituitary adenoma, hypothalamic disorders, or hyperthyroidism. Prolactin has been reported to directly affect adrenal androgen secretion.
Iatrogenic hirsutism
It may be a side effect of systemic use of various drugs such as testosterone, danazol, oral contraceptives (less than 5% of cases), adrenocorticotropic hormone (ACTH), phenothiazines, minoxidil, metyrapone, cyclosporine, and synthetic glucocorticosteroids.
Pregnancy
Pregnancy rarely causes hirsutism. In such cases, hypertrichosis occurs due to the development of polycystic ovarian syndrome or virilization of tumors during the first or third trimester.
Hirsutism in postmenopause
The cause is unclear. Possible causes include ovarian or adrenal tumors and hypertrichosis or hypertrophy of the ovarian stroma.
History and physical examination are extremely important and critical in differentiating idiopathic hirsutism from other forms of the disease. Laboratory tests and ultrasound may be added if necessary.
Assessment of hair growth rate using the Ferriman-Gallwey scale in each of the 11 androgen-dependent areas (upper lip, chin, chest, upper back, lower back, upper and lower abdomen, shoulders, forearms, thighs, lower legs). The scale is four-point, with "0" indicating no hair growth. If the total score is 8 or higher, a diagnosis of hirsutism is made.Physical and chemical measures
Physical and chemical measures are used when both expectations and practical options are limited, such as in cases of mild familial or idiopathic hirsutism.
- Hair bleaching: This is an excellent, simple and inexpensive method used primarily by women with fair skin.
- Shaving: This is the most common method of removing unwanted hair from the legs and bikini line. It is also occasionally used to remove facial hair.
- Tweezing (Plucking): An easy, inexpensive, and safe method of removing isolated hairs, especially around the eyebrows, chin, and nipples.
- Waxing: Widely used to remove hair from the legs and upper lip. Must be repeated every 2 to 6 weeks.
- Depilatory creams: The main ingredient used is 5% calcium thioglycolate. This method is not recommended for women with fair skin or allergies because it can cause allergic contact dermatitis. Other common side effects include recurrent folliculitis and hyperpigmentation.
Systemic Treatment:
Systemic treatment includes the use of androgen receptor antagonists, 5α-reductase inhibitors, drugs that can suppress ovarian function, and corticosteroids.
- Cyproterone acetate (CPA): This medication inhibits the binding of testosterone and dihydrotestosterone to androgen receptors and increases the metabolic clearance rate of testosterone by stimulating liver enzymes and reducing sex hormone-binding globulin levels. CPA is a potent progestogen, but it should be prescribed with cyclic estrogen to reliably block ovulation. Therefore, it is prescribed with either 0.050 mg ethinyl estradiol from day 5 to day 26 of the cycle or 0.035 mg ethinyl estradiol from day 1 to day 21 of the first cycle and from day 5 to day 26 of subsequent cycles. The drug is usually prescribed for at least 2-3 years. Side effects may include decreased libido, breast tenderness, nausea, headache, depression, emotional disturbance, weight gain, and increased blood pressure.
- Spironolactone: This is a steroid androgen receptor antagonist that can also block the activity of 5α-reductase and, in high doses, reduce cytochrome P450 activity. It is prescribed at a dose of 50-200 mg/day for at least 6 months. After 12 months of use, an 83% reduction in facial hair has been observed. Side effects are generally mild and may include menstrual cycle disturbances, decreased libido, breast tenderness, headache, dizziness, nausea, vomiting, anorexia, diarrhea, hyperkalemia, and increased serum creatinine. The drug may also cause skin side effects.
- Flutamide: This is a pure nonsteroidal antiandrogen that has no glucocorticoid, progestational, androgenic, estrogenic, or antigonadotropic effects, both in vivo and in vitro. The active metabolite of flutamide, hydroxyflutamide, blocks the androgen receptor of the hair follicle target organ. It is usually administered at a dose of 250-375 mg/day for a period of 6 to 24 months. Improvement is usually seen after 3 months of use. Doses above 500 mg/day may cause toxic hepatitis and gastrointestinal disturbances.
- Finasteride: It is a potent type 2 5α-reductase inhibitor. It is used in women with facial hirsutism at a dose of 2.5 mg/day in combination with oral contraceptives for 2 years. The results are good and comparable to those obtained with CPA. Finasteride may cause feminization of male fetuses and may increase cholesterol levels when used in combination with oral contraceptives.
- Oral contraceptives: These work by suppressing ovarian function. They usually consist of a combination of estrogen (ethinyl estradiol) and progestin (ethinyl estradiol diacetate, lynestrenol, norethindrone acetate, norgestrel, desogestrel, norethynodrel, or levonorgestrel). The action of estrogens is mainly based on stimulating the production of sex hormone-binding globulin, which leads to a reduction in free testosterone levels. Oral contraceptives can also alter the binding of dihydrotestosterone (DHT) to its receptor and, with long-term use, reduce 5α-reductase activity. Oral contraceptives are contraindicated in women with thromboembolism, breast or uterine cancer, and hypertension.
- Gonadotropin Releasing Hormone Antagonists: Nafarelin and leuprorelin, synthetic analogues of gonadotropin-releasing hormone (GnRH), have been used successfully in the treatment of hirsutism. They work by reducing the production of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) in the pituitary gland. Triptorelin is a newer GnRH antagonist that has recently been used in the treatment of hirsutism.
- Corticosteroids: This is the treatment of choice for congenital adrenal hyperplasia. Corticosteroids lower plasma androgen levels. Prednisone is used at a dose of 7.5 mg/day for 2 months, with a dose reduction to 5 mg/day for the next 2 months, and finally to 2.5 mg/day for the following 2 months.
Electrolysis: This method is widely used to remove undesired hair. Electrolysis is performed with individual isolated and non-isolated epilation needles that are inserted into the hair follicle. The most common, although rare, side effects are hyperpigmentation and scarring.
Photodynamic therapy: This method, which uses aminolevulinic acid (ALA), is primarily used to treat skin neoplasms. Since ALA is absorbed by the hair follicles, the application of infrared light can cause selective damage to the cells and destruction of unwanted hair.
Laser: The use of lasers to treat excessive growth of unwanted hair is based on the principle of selective photothermolysis. This method does not provide a definitive solution to hirsutism, as hair regrowth is observed in the first 3-6 months. The main goal of laser hair removal is to increase the temperature in the hair follicle to 200°C in order to destroy it. This method is mainly used in cases of idiopathic hirsutism.
Alternative and experimental treatments: Recently, a new drug has been used to treat some cases of hirsutism. Eflornithine hydrochloride acts as an irreversible inhibitor of ornithine decarboxylase, an enzyme required for the synthesis of polyamines from dihydrotestosterone, which is necessary for the proliferation of hair matrix cells. The drug affects the rate of hair growth, but unfortunately provides only temporary hair removal.